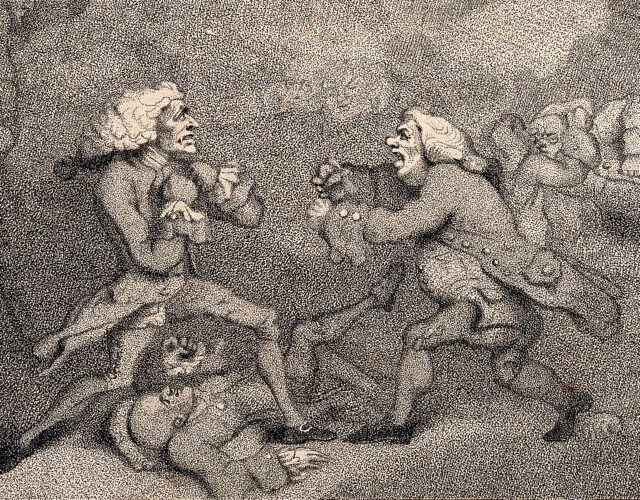
Normally, we think of doctors as healers, but over the centuries some have sought to inflict pain as well—particularly on each other.
Brawls between doctors were alarmingly common in the past, especially in the Americas. In the early 1800s the United States turned out five times as many doctors per capita as some European countries, sparking fierce competition for patients. Doctors beat each other bloody all the time for stealing business. As one Philadelphia physician said, his colleagues lived “in an almost constant state of warfare, quarreling, and . . . street fights.”
Sometimes these fights escalated into duels, the most notable of which took place in Jamaica in 1750. Nowadays, dueling often has a romantic air about it, but the participants were frequently violent buffoons who escalated petty squabbles into disputes over “honor.” This duel was no different. It involved swords, guns, a cowardly ambush, even insults in rhyming verse. But the duel did have one notable feature, in that its trigger was a mysterious blood disease, a disease that also played a significant role in expanding slavery in the Americas.
In 1750 a doctor in Jamaica named John Williams published a pamphlet on yellow fever, a disease that gets its name from the jaundice it can induce, which leaves victims’ eyes and skin looking yellow. Alarmingly, the afflicted sometimes vomit black blood as well—“like the grounds of coffee mixed with acrid unfinished bile,” as Williams described it.
Williams had encountered yellow fever as a doctor on slave ships sailing back and forth across the Atlantic. After profiting off human misery for several years, he settled in the slave port of Kingston in the 1740s, where he continued to aid and abet the trade. In his spare time, he also began studying yellow fever in earnest.
In his pamphlet, Williams described yellow fever in general terms, but certain passages stirred up trouble. First, Williams waded into a long-standing controversy about yellow fever’s origins. Most Europeans believed it had originated in the Americas and spread from there to Africa. Williams thought the opposite—that it had originated in Africa and been imported to the Americas.
We now know Williams was correct. Yellow fever first arose thousands of years ago in Africa. After European contact with the Americas, the virus crossed the Atlantic in ships, either in stowaway mosquitos or in the blood of sailors or African slaves. But at the time, Williams’s ideas provoked people.
The controversy was particularly intense because in some ways it was a proxy for a larger dispute about the relationship between Europe and the Americas. Europeans typically held condescending views about the “New World” and preferred thinking of their colonies abroad as wild and primitive places, rife with strange diseases. Nor did most Europeans want to acknowledge their role in spreading diseases to new lands.
The pamphlet’s second controversial point involved a mysterious tropical disease called blackwater fever. Among other ghastly symptoms, people with blackwater fever sometimes urinated blood. It reportedly looked like borscht soup.
Given that yellow fever involved vomiting blood and blackwater fever involved peeing blood, people naturally linked the two. In fact, many claimed that yellow fever and blackwater fever were different manifestations of the same disease.
Williams, however, provided strong evidence against this idea. Specifically, that “Peruvian bark” did not cure yellow fever, whereas it did cure blackwater fever. By Peruvian bark, Williams meant the bark of the cinchona tree from South America, history’s first effective treatment for malaria and the eventual source of quinine, which was isolated in 1820.
Because Peruvian bark cured blackwater fever, Williams argued that blackwater fever was simply an extreme form of malaria. Once again, history proved him right. Malaria breaks down red blood cells in the body, and sometimes so many red blood cells break down that people pass them in their urine.
If Williams had stopped there, he would likely be remembered today as a smart if minor player in the history of tropical medicine. (Other doctors were mixing up yellow fever and blackwater fever as late as the 1870s.) Unfortunately for him, Williams did not stop there. He was arrogant, condescending, and had a wicked tongue. In his pamphlet he dismissed those who disagreed with him as fools and idiots.
He especially scorned doctors who had received their medical training at universities. Instead of working with patients, he wrote, they filled their heads with “whimsical notions” from antique books. Worse, they fed their patients “occult venoms” and other so-called remedies that did more harm than good.
In contrast, Williams portrayed himself as having real-world experience with tropical diseases. He claimed that anyone in Jamaica who visited a European-trained doctor instead of him was a “blockhead.” Once again, it boiled down to competition for patients.
Naturally, these insults angered Jamaica’s European-trained doctors—especially one hothead named Parker Bennet. Bennet was roughly 25 years old in 1750, Williams’s junior by about 15 years, and like Williams, he had happily worked on slave ships for years. But before that, he’d undergone exactly the sort of expensive university training Williams scorned. So Bennet returned fire on Williams in a pamphlet of his own. He pointedly referred to his adversary as Mister Williams over and over, to highlight Williams’s lack of a medical degree. The implication was clear. Visiting Mr. Williams for treatment was dangerous. Instead, come see Doctor Bennet.
Williams felt honor-bound to answer this insult. And incredibly, he did so in heroic couplets, as if channeling Alexander Pope: “Bennet, whose trifling writings no point hit / That fop in learning, and that fool in wit.” Insults back then had style.
Naturally, Bennet answered back, albeit in an essay. He opened with a not-very-subtle line from Psalms: “The mouth of them that speak lies shall be stopped.” Then he mocked Williams for, quote, “bad poetry, false measure, and vile logic.” For good measure, he called Williams a “conceited dunce” and a “cringing fop.” And after all that, he also accused him of killing patients with opium.
It’s not clear who challenged whom, but rather than marshal evidence or talk things through like mature adults, the doctors decided to duel.
It was a wild affair. Eager for violence, Bennet showed up at Williams’s house early on the morning of December 29, 1750, armed with a sword and pistols. He handed the weapons to a young servant he’d dragged along, then marched up and pounded on Williams’s door, demanding to hold the duel then and there.
Spying from an upper balcony, Williams realized Bennet was momentarily unarmed. And rather than hold a fair fight, he decided to get the drop on his enemy. He grabbed his own pistols and sword, crept down to his front door, and opened it just a crack.
Quick as a flash, he darted his gun out and fired. The shot caught Bennet in the chest.
Thankfully for Bennet, Williams was not firing a metal slug; instead, he used so-called goose shot, which consisted of small bits of lead, like tiny BBs. Still, the shot hurt. Bennet lurched back from the door and ran toward his servant boy, who stood in the yard with the weapons.
But Bennet wasn’t quick enough. Williams unchivalrously fired his second pistol at Bennet’s back, nailing him in the knee with more goose shot.
Bennet staggered up to his no-doubt-terrified servant and grabbed his sword. But the sword got stuck in the scabbard, and Bennet could not dislodge it. As one contemporary chronicler put it, he “begged of God to invigorate him a few moments.” But like the fabled sword in the stone, it would not budge.
While Bennet was busy praying, Williams was bearing down on him with his own sword. With a yell, he stabbed Bennet in the chest and pierced both lungs. It was a fatal blow—but not immediately fatal.
Maybe Williams’s blow loosened the stuck sword. Or maybe God finally answered Bennet’s prayer. Whatever the case, in that moment Bennet’s sword popped free from the scabbard. Despite his mortal wound, all his thoughts were still bent on violence, and he lunged and struck Williams just beneath the collarbone. The steel tore through Williams’s jugular vein, causing a burst of blood in his throat.
With blood pooling in his lungs, Williams staggered toward his house, gurgling. He made it only a few steps before collapsing dead.
Bennet lived for another few hours, writhing in agony until he succumbed. It was a rare duel with two deaths.
What’s often lost in the many retellings of this story over the years is the larger context—why the debate over yellow fever and malaria mattered so much in Jamaica and other colonies. To a large degree, it comes down to slavery.
Both Williams and Bennet had worked on slave ships, and Kingston was a major slave port, where captured Africans landed before being shipped to plantations in the Caribbean and North America.
In the early days of colonization, however, plantation owners had leaned heavily on two other groups for labor: indigenous peoples, who were also often enslaved; and indentured servants, poor Europeans who worked for a fixed length of time before being freed.
At first, indigenous peoples and indentured servants made up a significant fraction of the plantation workforce in the Americas. However, many of them died from tropical diseases, especially yellow fever and malaria. Colonial doctors struggled mightily to lower that death rate and were desperate for any bit of understanding to help fight those diseases.
Africans also died from yellow fever and malaria, of course. Crucially, though, they died at far lower rates. That’s because many had been exposed to the diseases back home, and the survivors had built up immunity. People from sub-Saharan Africa were also more likely to have advantageous genetic adaptations, such as sickle-shaped red blood cells that resist parasite infections. As a result of that immunity—and the impotence of European doctors—the African slave trade expanded rapidly. As more and more indigenous and European workers died of yellow fever and malaria, Africans bore the brunt of the oppression, and the slave trade grew to apocalyptic scales—ensnaring at least 10 million men, women, and children.
Williams and Bennet were just two of the many, many casualties wrought by yellow fever and malaria. But unlike so many innocent men, women, and children, they had only themselves to blame.